
The elbow may be known as the “funny bone” but if you suffer from tennis or golfer’s elbow, the pain you feel is no joke. Read on to discover why it hurts — and what you can do to regain comfort, mobility, and top performance.
++
Your elbow may not look remarkable. (In fact, it’s kinda hard to get a good look at your own elbow in the first place.)
Yet multiple muscles, tendons, nerves, and ligaments all vie for space in that one small square. And while nature’s tight packing job gives the joint stability, connective tissue congestion can also create smash-ups.
Make a fist and move your wrist around. Bend and straighten your arm. Try opening a jar, or squeezing a tennis ball. Any elbow pain from any of these activities? If so, you’re in good company.
About 1-3 percent of people suffer from tennis or golfer’s elbow. And in one survey as many as 5 percent of workers reported that they’d taken a sick day because of elbow pain in the past year.
Even more, nearly 29 percent of people in jobs that involve repetitive gripping and wrist flexion suffer from tennis and golfer’s elbow. This includes everyone from lumberjacks to cooks to professional bodybuilders to meat processing factory workers.
Other factors associated with developing tennis and/or golfer’s elbow include:
- Being female
Women tend to have more joint inflammation and laxity than men. - Getting older
Connective tissues heal less well as we age, and we build a history of cumulative movement trauma. - Being overweight
Fat tissue, in excess, secretes inflammatory chemicals. - Smoking
This prevents oxygenation and blood flow to tissues. - Handling loads repetitively, especially for longer periods
The stress creates an ongoing demand that your joints can’t recover from. - Repetitively bending/straightening the elbow
Actions like putting things on a shelf or scanning groceries cause wear and tear. - Getting into lots of fistfights
Just kidding… kinda.
What is tennis or golfer’s elbow?
Obviously, you needn’t be a golfer or tennis player to have elbow pain.
The terms “tennis elbow” or “golfer’s elbow” simply refer to a type of pain that appears either on the outside (lateral) or inside (medial) of the elbow.
Or in some unlucky people’s cases — both.
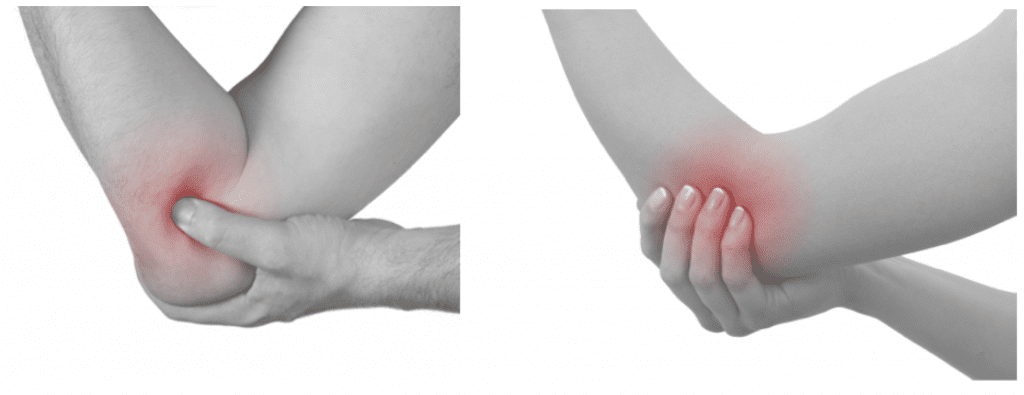
Tennis (lateral epicondlylitis) and golfer’s elbow (medial epicondlylitis) tends to feel like a dull ache in the elbow joint that gets worse with more activity.
Usually the pain is relatively localized — there’s a specific spot that is painful, and it’s aggravated by gripping and bending and/or straightening the elbow.
However, in serious cases, the pain can extend down the forearm, or up into the biceps and triceps, as more nerves are aggravated. This pain comes from chronic damage to and/or inflammation of nerves and soft tissues in the joint.
What causes elbow pain?
Most cases of tennis or golfer’s elbow are caused by structural changes in the tendon. That shouldn’t really come as a surprise, since up to 50 percent of sports injuries involve tendons.
Lack of mobility, poor mechanics, overuse, and/or muscle imbalances can all contribute to these structural changes.
How do tendons work?
Tendons attach muscle to bone and help create elastic energy in the joint.
They’re mostly water (68 percent) along with connective tissue proteins such as type 1 collagen, glycosaminoglycans (which help to absorb shock), and elastin.
When a tendon is overused and/or stressed, it can become shortened, develop adhesions, inflame, and break down.
We also don’t produce connective tissue proteins as quickly as we age. We get more stiff and less springy. So we tend to have more joint pain as we get older, because we’re not rebuilding stressed tissues as rapidly as a younger person might.
Tendons heal slowly after breaking down because they don’t have a good supply of blood vessels.
Blood, oxygen, and nutrients take a long time to find their way into connective tissues. In fact, tendon healing after an injury can take as long as two years!
The importance of recovery
It might seem counterintuitive, but regular movement and mobility work is important for joint health. Movement tells the joint to keep lubricated and producing valuable proteins, and helps deliver nutrients to joints.
But the movement has to be varied in type and loading (rather than always repetitive and/or heavy), and not overload a joint’s ability to recover.
In the first 24 hours after exercise, collagen synthesis and breakdown both increase. We temporarily lose collagen during this time.
However, in the 48 hours that follow, this breakdown decreases. We get collagen rebuilding and synthesis. Synthesis means healing.
So, if we’re continually hammering our tendons with hard exercise, they’ll be in a continual state of breakdown and never get a chance to heal. Pain and dysfunction inevitably follow.
Kind of reinforces the idea of taking a day off between heavy training sessions, huh?
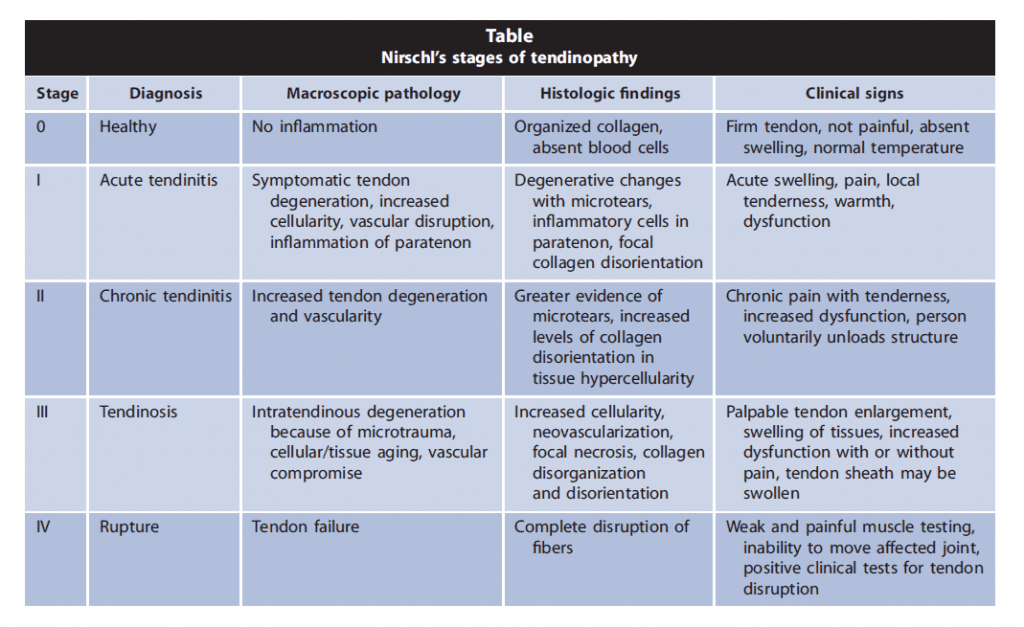
As you’ll see in the chart below, tendon injuries can progress from minor inflammation or microtears to complete tendon failure.
This process is usually cumulative — it means you’ve been stressing your joints and often ignoring minor pains that signal earlier stages of damage.
Golf pain or tennis pain: What’s the difference?
Sixteen muscles cross the elbow joint along with a nest of ligaments, nerves, and blood vessels.
Muscles that flex your wrist attach to the medial epicondyle (a.k.a. one of the bumps at the end of the bone). Muscles that extend your wrist attach to the lateral epicondyle.
(Quick note: “Medial” refers to things closer to the midline of your body, while “lateral” refers to things farther away from the midline. So the inside of your arm is medial, while the outside of your arm is lateral.)
In both cases, the injury comes from repetitive stress — usually gripping plus either bending the elbow (as in tennis) or straightening the elbow (as in golf).
Medial pain
Medial elbow pain can result from a medial collateral ligament injury, ulnar nerve irritation, a bone issue, or problems with the flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), palmaris longus (PL), or pronator teres (PT) muscles.
Anyone who repetitively contracts the flexor-pronator muscles without giving them time to regenerate might run into this problem. Golfers, bowlers, racquetballers, footballers, weightlifters, carpenters, and overhead throwing athletes are at particular risk.
Lateral pain
Lateral epicondyle pain occurs up to 10 times more often than medial epicondyle pain. And it’s been recognized at least since the 19th century. It was then that doctors first noticed it in people who played lawn tennis — hence its common name.
Interestingly, novice tennis players tend to get tennis elbow more often than experienced players, likely because they over-grip, aren’t strong enough in foundational muscles and connective tissues, and have otherwise poor playing mechanics.
Meanwhile, older women who play tennis tend to suffer more from tennis elbow if they do a lot of knitting, macramé, and gardening – all activities that can put similar stress on the joint.
Lateral elbow pain can result from a lateral collateral ligament injury, radial nerve irritation, arthritis, folds in tissues, loose cartilage, or problems with the anconeus (AN), extensor carpi radialis brevis (ECRB), extensor carpi radialis longus (ECRL), extensor carpi ulnaris (ECU), or extensor digitorum (ED).
Gripping, rotating the palm towards the face, and trying to flex the back of the knuckles towards the wrists (for example, when taking the hands off of a keyboard) will be painful actions for anyone suffering from tennis elbow.
Non-surgical treatment for elbow pain
Let’s start with the most groundbreaking treatment method: ice. Ice can be used to control pain and inflammation. Tell your friends you heard it from me first.
But if ice isn’t enough, your doctor may request an MRI to show the extent of changes to ligaments, tendons, muscles, and bones, while also revealing any changes to the bone itself.
ECSW (extracorporeal shock wave) therapy and ultrasound may help reduce pain and promote tissue regeneration. ECSW appears more useful for lateral elbow problems than for medial problems.
Elbow bands seem to help the rehab process. Bands reduce tension on muscles below where they’re placed by distributing the stress across more tissues. Thus, a band just below the elbow can ease pain.
Eccentric exercise is the phrase we use to describe the lowering or “negative” phase of a movement. (An example would be the “down” part of a biceps curl, where you resist the weight just enough to lower it slowly.) Eccentric exercise is often prescribed for elbow injuries and pain, since it encourages the remodeling of tissues.
Eccentric exercise places greater tension on muscles and tendons. Meanwhile, it limits the body’s production of waste products that can irritate tissues. This is a good thing for promoting a healing environment. You can watch a video that summarizes the research about this here.
If you use eccentric movements for tendon rehab, aim for a load that allows 4 sets of 15 (or up to 30) repetitions with no “bad” pain. If you feel pain, back off and try again. Between 3 and 7 total sessions per week should include the rehab exercise of choice done after a brief warm up.
But please note: Do not perform concentric motions during an eccentric rehab protocol. Weight should be returned passively to the starting position. This means you may have to assist yourself back to the starting position. Concentrics can begin again once you can perform your normal daily activities without pain.
Platelet rich plasma (PRP) therapy shows some promise for degenerative injuries at the elbow. Why? Because platelets contain compounds that initiate and promote healing. (This is why platelets migrate to the site of an injury in the body.)
Some PRP therapies also contain white blood cells, or WBC. It’s unknown if this is useful or not. While WBCs do help with tissue repair, they also might stimulate too much inflammation at the injury site.
Massage, stretching, and active release therapies (ART) may reduce symptoms and promote recovery in tendonopathies.
Compression therapy may help bring an influx of blood and nutrients to the area. Some folks like an elbow compression sleeve, which provides both mild compression and proprioceptive (touch) cues that help people know what the joint is doing, and that may interfere with pain signals. Other folks like a more extreme compression — wrapping the joint very tightly (e.g. with elastic banding or a tight fabric bandage) for a minute or two, then unwrapping it to let blood rush back in.
However, be careful. According to elbow expert Eric Cressey, aggressive compression could be a problem for people with an ulnar neuritis or thoracic outlet presentation. In fact, he discourages throwers from using extreme compression on elbows because of all the nerves exposed in the elbow joint. The lower body is a different story, though.
Acupuncture and Botox are also sometimes proposed, but there isn’t an overwhelming amount of evidence showing benefits from these.
NSAIDs can help in the acute phase to reduce pain, but it’s important not to use them to push through pain because this will only lead to greater dysfunction. NSAIDs used for a long time can also cause gastrointestinal upset – and you probably don’t want to add stomach pain to your elbow pain.
Corticosteroids are also sometimes prescribed. Like NSAIDs, these do nothing directly to help in recovery. They can be useful during the rehab process to reduce pain, but in the long run they can have some undesirable side effects and it’s better not to rely on them.
Nitric oxide may help connective tissue production. But it seems to work best when a patch is placed directly on the injury. It’s hard to say if eating foods and supplements that promote nitric oxide production in the body would offer much in the way of help. (In case you want to try it, examples include watermelon, beets, celery, arginine, and garlic.)
Cressey also suggests that a lot of tennis elbow situations could be related to a chronic forward head posture. So he encourages everyone with chronic lateral elbow pain to get their neck screened – by working with a chiropractor, physical therapist, or manual therapist – just to be safe.
Surgery
Surgery is a last resort. But it can be used, and if 12 months of non-operative treatment fails, then it’s probably worth investigating.
Eating for tendon health
Regardless of what treatment option you choose, support your connective tissues’ health with a nutrient-rich, low-inflammation diet.
- Eat plenty of colorful fruits and vegetables.
- Eat enough protein, which provides the “building blocks” of tissue repair.
- Consider supplementing with vitamin C, vitamin A, zinc, and copper if you are deficient.
- Consider anti-inflammatory foods and supplements such as ginger, turmeric, and/or an omega-3 supplement.
- Limit inflammatory foods (such as processed foods and sugar) as well as any foods to which you know you’re intolerant.
In PN’s Women’s Coaching, Men’s Coaching, and Certification programs, we also teach about how to eat in a way that promotes overall health and recovery.
What to do
Be smart
If elbow pain bothers you for more than a couple of days, and ice and rest don’t cure it, see your health care provider. You know you need to set up an appointment. Just do it.
Check your repetitive motions — whether job or exercise or sport related. If you are in pain, you are probably doing too much. How many swings, pitches, etc. are you doing each day? How much grip work?
If you beat up your tendons day after day, you’ll probably suffer for it.
Work out smart
- Try a safety bar squat or a cross arm (“genie”) front squat instead of regular barbell back squats to decrease elbow stress.
- Do fewer isolation exercises for biceps and triceps. Instead, focus on compound exercises where the load is higher and the stress is distributed over more than one joint.
- If it hurts, avoid it. Find an alternative.
- Vary your movements and loading. Take a day off between intense workouts. Build in recovery days each week with easy movement and mobility work. Have a diverse roster of activities instead of doing the same handful of things over and over.
- You can use an elbow band if you find it comfortable during workouts.
- Try lifting straps to decrease the amount of gripping necessary for heavy lifts, like this.
- Look at overall upper body mobility. A tight posterior shoulder capsule may contribute to elbow pain.
- Build a solid foundation and mechanics before you increase the speed or resistance at which you do something. Remember that connective tissues take a long time to build and heal.
Live smart
- Check your computer workstation. If your hands are always in pain, change the setup.
- Get massage therapy and work on flexibility. Try some regular forearm soft tissue work.
- Engage in rehab with pain free strengthening exercises (wrist curls, reverse wrist curls, elbow flexion, elbow extension, forearm pronation/supination).
- Return to full-strength activities gradually. You may need as much as a year of rehab exercises.
Eat smart
Try the following foods and/or supplements that help to moderate inflammation and promote tissue healing:
- Foods/supplements rich in omega-3 fats:
Algae oil, flax, chia, hemp, walnuts, leafy greens, fish, fish and marine oils (e.g. krill and algae)
- Foods/supplements rich in flavanoids:
Turmeric, garlic, pineapple, tea, berries, cocoa
- Foods rich in vitamin C:
Guava, red bell pepper, broccoli, green bell peppers, strawberries, grapefruit, kohlrabi, papaya, Brussels sprouts, kiwi, mango, oranges
- Foods rich in vitamin A:
Carrots, pumpkin, sweet potato, spinach, collards, kale, watercress, beets, winter squash, tomatoes, dried apricots, mango
- Foods rich in zinc:
Mushrooms, spinach, sesame seeds, pumpkin seeds, green peas, baked beans, cashews, whole grains, oysters, chicken, crab, lamb, beef, pork, turkey, lobster, wheat germ, watermelon seeds
- Foods rich in copper:
Mushrooms, green leafy vegetables, barley, soybeans, tempeh, sunflower seeds, navy beans, garbanzo beans, cashews, molasses, beef liver, oysters, lobster, crab, chocolate, cocoa powder.
- Amino acids:
Supplementing with arginine (7 grams, 2x/day), HMB (1.5 grams, 2x/day), and glutamine (7 grams, 2x/day) might assist in collagen deposition and injury healing.
Also, try keeping a food journal as well as tracking your pain / inflammation symptoms.
See if you notice any correlations. When is your pain better or worse? Do particular foods seem to make a difference?
Many people find that when they remove inflammatory foods, and/or foods to which their body reacts, they have less joint pain.
Eat, move, and live… better.©
Yep, we know… the health and fitness world can sometimes be a confusing place. But it doesn’t have to be.
Let us help you make sense of it all with this free special report.
In it you’ll learn the best eating, exercise, and lifestyle strategies – unique and personal – for you.
Click here to download the special report, for free.
References
Click here to view the information sources referenced in this article.
Share